Luke Seppi, Lynn Worobey PhD, Adam Popchak DPT, Michael Boninger MD
Human Engineering Research Laboratories, Department of Veterans Affairs, Pittsburgh, PA; Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA
ABSTRACT
Many people expose themselves to activities that can be harmful to their shoulders, especially wheelchair users. Altered scapular kinematics has often been linked to shoulder pain and pathology. Eighteen subjects’ scapular movements were examined using a novel freehand three-dimensional ultrasound technique. Upward rotation, external rotation, and posterior tilting increased with humeral elevation angle. Clinical exam scores that evaluate shoulder health and subject characteristics, such as body mass index, were correlated to decreased upward rotation and posterior tilting. Results indicate that this ultrasound based method could be applied to evaluate scapular kinematics in different populations where shoulder pathology is prevalent.
BACKGROUND
Shoulder pain, dysfunction, and pathology are prevalent among the wheelchair user population due to the repetitive movements, awkward postures, and high forces associated with daily activities such as wheelchair propulsion and transfers [1]. Shoulder pain and pathology limit mobility and independence in activities of daily living, such as dressing, feeding, transfers, and hygiene [2]. Prevention of shoulder pathology in wheelchair users is of utmost importance because of the debilitating nature of the condition and the poor outcomes from conservative and surgical treatments [3,4,5]. It has been demonstrated that people who experience shoulder dysfunction and pathology often have altered scapular kinematics [6]. Evaluation of scapular kinematics could be a useful means to identify shoulder problems and could lead to early interventions. Several methods of evaluating scapular kinematics are currently available but limited by potential harmful effects or lack of dynamic testing ability. X-rays were among the earliest methods of investigating scapular kinematics, but they expose patients to high levels of radiation and can only take images of static positions. Bi-planar radiography is another method that exposes subjects to radiation and while better than x-ray, its use still needs to be validated in populations of interest. Magnetic resonance imaging (MRI) provides very high quality images, but is expensive, requires a large machine, and may not allow subjects to complete dynamic tasks in functional positions during testing. Bone pins are highly effective in tracking scapular movements, but are invasive, which has limited sample sizes. Digitizers are both non-invasive and safe, but they lack measurement accuracy and can only be used to analyze static positions [7,8,9]. Electromagnetic sensors have also been used but are generally limited in accuracy at higher angles of arm elevation.
This study presents a new non-invasive and safe method for evaluating scapular movement using freehand three-dimensional ultrasound. This method pairs ultrasound with motion capture to image the borders of the scapula and characterize scapular movement.
METHODS
Subjects
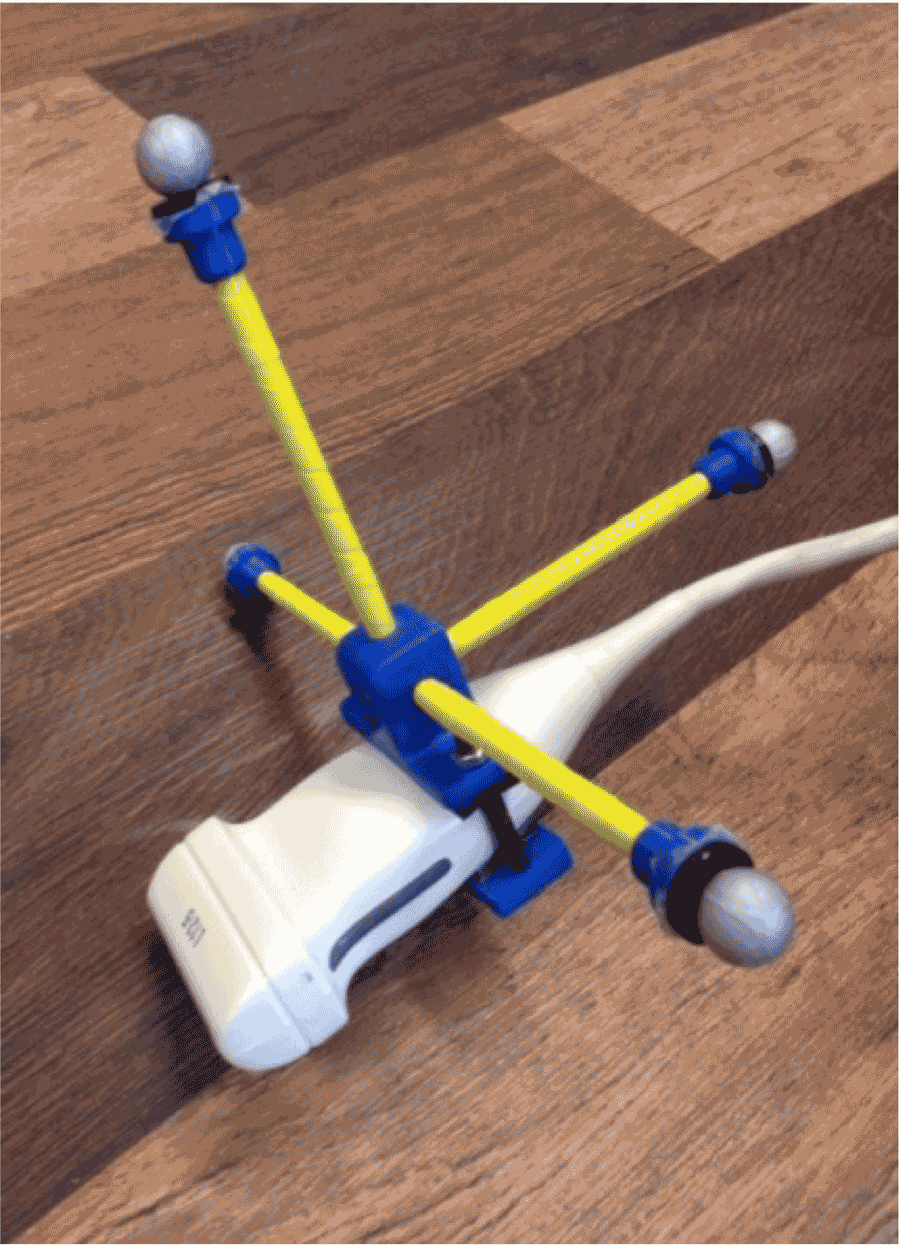 Figure 1: Ultrasound probe fitted with the custom orthogonal attachment with Vicon markers.
Figure 1: Ultrasound probe fitted with the custom orthogonal attachment with Vicon markers. Subjects were able to participate if they were at least 18 years old, spoke English, and were able to raise their dominant arm above their head. Subjects were ineligible if they suffered from upper extremity impairment, weakness or spasticity that didn’t allow smooth movement of the arm, if they were unable to accomplish reach tasks while seated with support straps, or if they had any lingering fractures or dislocations in the shoulder. Subjects included both wheelchair users and able-bodied controls.
Testing Setup
A custom testing chair was built with torso and shoulder restraints to isolate dominant shoulder scapular movement during ultrasound scanning. An adjustable guide bar was attached to the chair in the scapular plane to guide arm elevation. Vicon markers were placed on the trunk and dominant arm using the following bony landmarks: C7, T8, anterior sternoclavicular (sternum), processus xiphoidesu (xyphoid), anterior acromioclaviculare (acromion), lateral epicondyle, and medial epicondyle [10]. A custom orthogonal attachment was built with 4 Vicon markers to track the ultrasound probe during testing (Figure 1). Ultrasound was collected using a Philips HD 11 XE ultrasound machine equipped with a 5-12 MHz linear transducer coupled with an Epiphan Frame Grabber. All movement was captured using Vicon Nexus software and 10 Vicon cameras.
Arm elevation trials
Subjects were instructed to raise their dominant arm with their palm against the guide bar and thumb pointed upward. A marker was placed on the guide bar at 90° of elevation to maintain consistency. The subject was directed to raise their arm to the marker over a 5 second period and then to lower it back to their side over another 5 seconds. Subjects rested for 10 seconds between repetitions to prevent fatigue. Subjects completed 20 repetitions, with the ultrasound probe held at a new location along the spine or medial border for each repetition. The multiple locations allowed us to reconstruct the movement at different aspects of the scapula for the entire range of motion.
Clinical Exam
Prior to testing, subjects underwent two clinical examinations of their dominant shoulder to determine if they had pathology. The Physical Exam of Shoulder Scale (PESS) tests for pain in various impingement syndromes with 11 items. Scoring ranges from 0 (symptoms of pain definitely absent for all items examined) to 22 (symptoms of pain definitely present for all items) [11]. The Ultrasound Shoulder Pathology Rating Scale (USPRS), which examines the bone and soft tissue of the shoulder, was also used. Scoring ranges from 0 (normal tendon fibrillar patterns and cortical surface, no evidence of impingement) to 20 (fuller thickness tendon tears and cortical irregularities, marked impingement) [11].
Data processing
A custom Matlab program was written to convert the trial ultrasound video (10Hz) to individual images. Another custom Matlab program was written to allow for manual identification of the most posterior aspect of the scapula in each image. Once the scapula was identified in the two-dimensional ultrasound images (Pbeam), a series of transformations were applied to reconstruct the scapular border in three-dimensional space based on a static calibration relating the ultrasound beam to the orthogonal attachment (TbeamS,attachS), the location of the probe during testing (TattachD,global), the position of the subject’s trunk at the time the image was collected (Tglobal,trunkD), and the average position of the subject during testing (TtrunkS,global):
P![]() global = [T
global = [T![]() trunkS,global][T
trunkS,global][T![]() global,trunkD][T
global,trunkD][T![]() attachD,global][T
attachD,global][T![]() beamS,attachS] * P
beamS,attachS] * P![]() beam
beam
A local coordinate system was defined for the reconstructed scapular border similar to ISB guidelines. We first fit a plane to the entire reconstructed scapular border for the x-axis. Then we fit a regression line to the points of the scapular spine for the z-axis. A YXZ rotation sequence for matrix decomposition was used to determine scapular rotation. Rotations were defined as follows: internal/ external rotation (y-axis), upward/downward (x-axis), anterior/posterior tilting (z-axis). Humeral elevation and trunk position were determined using ISB recommendations [10]. Scapular position was characterized at 30°, 60°, and 90° arm elevation. An example of the reconstructed scapular border for these elevation angles can be seen in Figure 2.
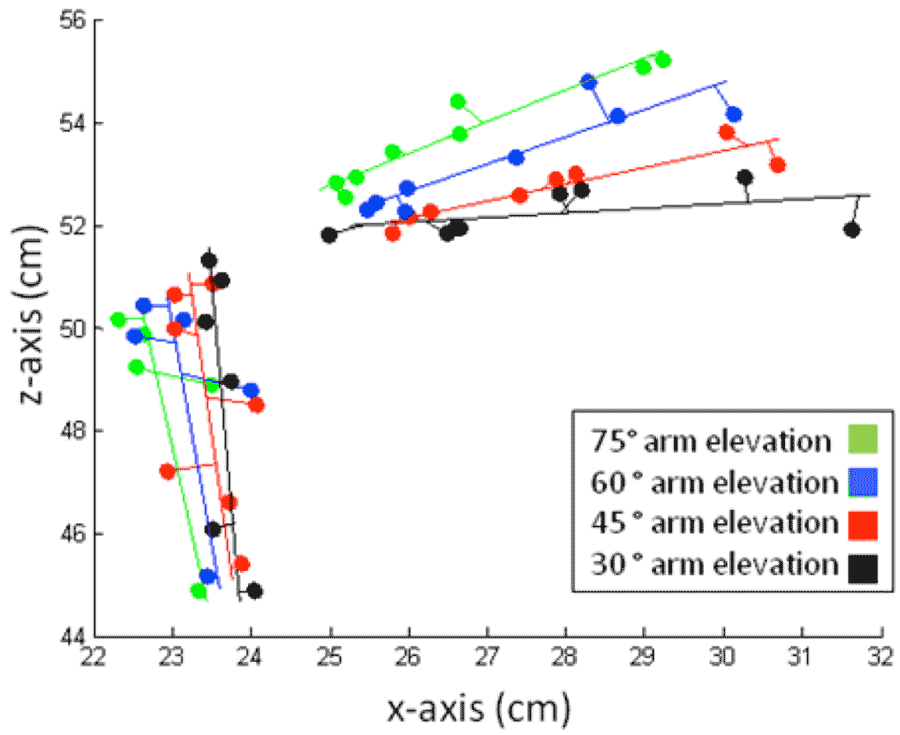 Figure 2: Reconstructed scapular border for different levels of arm elevation
Figure 2: Reconstructed scapular border for different levels of arm elevationComparisons were made between groups (able-bodied controls and wheelchair users) using Wilcoxon signed rank tests. Scapular rotations were compared for different arm elevations using the Friedman test with Wilcoxon signed rank tests to compare between consecutive elevation angles (30°,60° and 60°,90°). The relationship between USPRS/PESS scores with scapular rotation after the first phase of arm elevation (30°-60°) and second phases of arm elevation (60°-90°) were evaluated using the Spearman’s rank correlation coefficient. Statistical analysis was completed using IBM SPSS Statistics 20 with significant level set a priori at 0.05 with a Bonferonni correction for multiple comparisons.
RESULTS
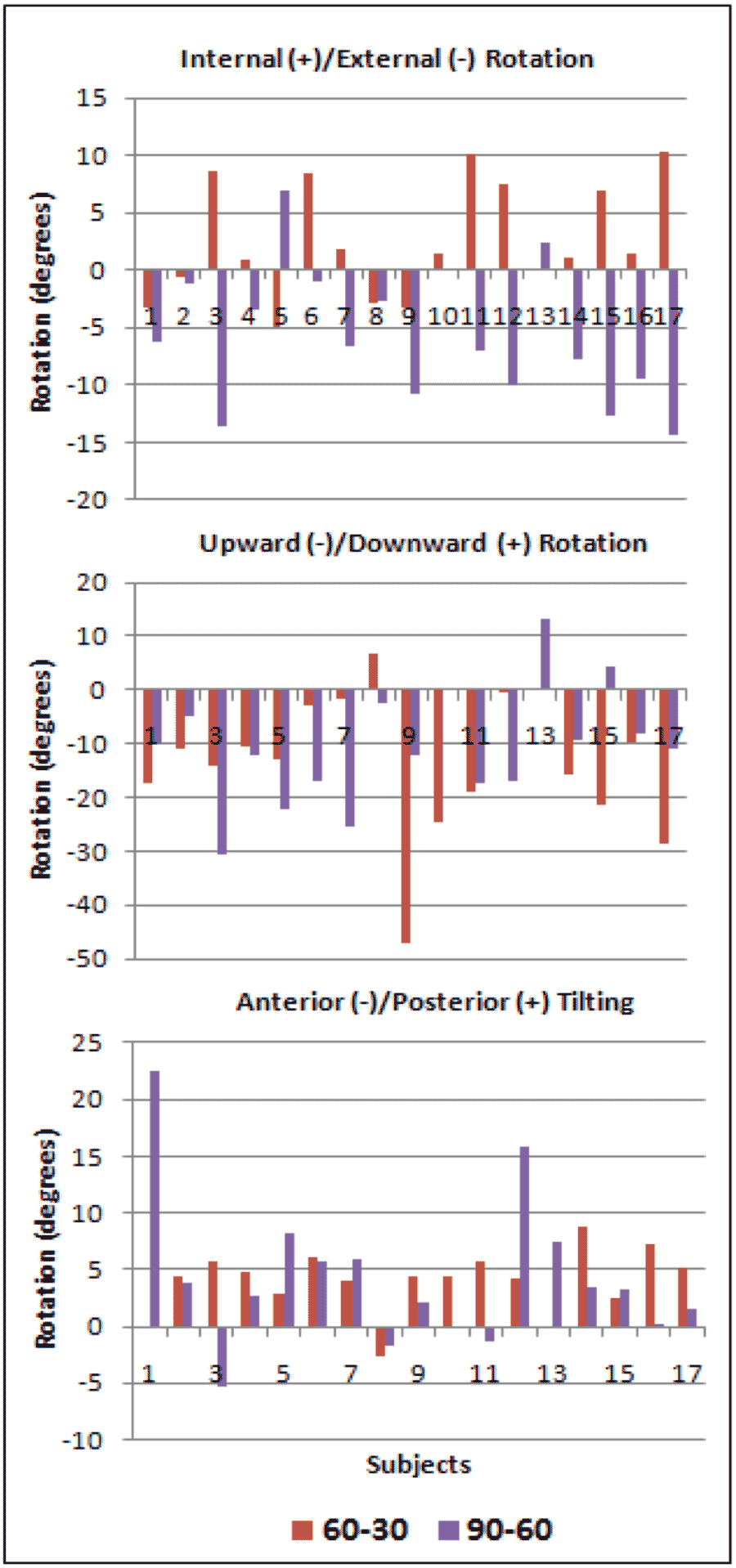 Figure 3: Differences in internal/external, upward/downward, and anterior/posterior rotations between 30°-60° and 60°-90° arm elevation
Figure 3: Differences in internal/external, upward/downward, and anterior/posterior rotations between 30°-60° and 60°-90° arm elevationA total of 18 subjects participated in this study, 9 of which were wheelchair users with an average of 16.6±10.2 years of wheelchair use. The participants were on average 51.2±9.1 years old and had an average BMI of 23.6±3.2. No differences in scapular rotations, age, or clinical exam scores were found between groups (p:0.093-0.963). The average PESS and USPRS scores for the subjects were found to be 1.6±1.9 and 4.8±3.5, respectively. We found a significant difference in scapular rotations at different levels of arm elevation (p<0.001). Post hoc comparisons revealed increases in upward rotation (p=0.001) from 30° to 60° and in posterior tilting (p=0.0004) and external rotation (p=0.004) from 60° to 90°. These increases are also demonstrated in Figure 3. Relating subject characteristics and clinical exam scores to scapular rotations, we found decreased upward rotation at 30° was correlated with increased PESS score (p=0.020). Posterior tilting at 60° also was found to decrease as the subject’s USPRS score increased (p=0.041).
DISCUSSION
In this study we were able to reconstruct the scapular border from ultrasound images and see a pattern of increased internal rotation, upward rotation, and posterior tilting as arm elevation increased throughout trials. These findings are consistent with patterns discovered by Ludewig, who used skin based electromagnetic tracking during dynamic movement [6]. We also determined that decreased upward rotation of the scapula was correlated with increased PESS score. A decrease in upward rotation is important to prevent as it decreases the clearance of the humeral head under the acromion, which can create impingement, and hence pain this finding is also supported by studies of Ludewig and Cook et al. [6] Posterior tilt decreased as USPRS score increased. Subjects with subacromial impingement tend to have decreased posterior tilt, as less posterior tilt also decreases the space between the acromion process of the scapula and the humeral head.
As freehand ultrasound has never before been used to evaluate the kinematics of a structure such as the scapula, the agreement of our results with other research demonstrates that our technique may be used in future evaluations of such body structures.
Future Work
Future studies should validate our freehand ultrasound technique by comparing results to an acceptable gold standard for evaluating scapular kinematics. A reliability study should also be conducted to validate the freehand ultrasound technique. After this technique is validated, future studies could compare the effects of loading on scapular kinematics or evaluate the effects of therapeutic interventions. Future studies may also extend to testing different body parts and joints, such as knees, wrists, ankles, etc. as well as different populations, such as overhead athletes.
Limitations
Limited sample size may have reduced our ability to detect a difference between groups. In addition, the dynamic sampling frequency of our frame grabber and the ability to capture quality ultrasound images caused us to down-sample our data and limited number of points in our reconstructed scapular border. As only 1 trial was completed per subject, During testing, many subjects did not reach the desired arm elevation of 120°, which limited us to only 90° and some studies have found greater between group differences at higher arm elevations. Lastly, the wheelchair users in this study had limited shoulder pathology which may have contributed to similar scapular rotations between groups.
CONCLUSIONS
This study used a new freehand three-dimensional ultrasound technique to evaluate scapular kinematics and found that consistent with previous studies, scapular rotations increased with humeral elevation. This study was also able to relate scapular rotations to clinical exam scores. The results support the feasibility of using freehand ultrasound to examine a moving structure in three-dimensions. A reliability study with a larger sample size, more trials, and a wider range of shoulder pathology should be conducted in the future.
REFERENCES
[1] van der Windt DAWM, Thomas E, Pope DP, et al. Occupational risk factors for shoulder pain: a systematic review. Occupational and environmental medicine. 2000;57(7):433-442.
[2] Silfverskiold J, Waters RL. Shoulder pain and functional disability in spinal cord injury patients. Clinical orthopaedics and related research. 1991;272:141.
[3] Bayley JC, Cochran T, Sledge C. The weight-bearing shoulder. The impingement syndrome in paraplegics. The Journal of bone and joint surgery. American volume. 1987;69(5):676.
[4] Robinson M, Hussey R, Ha C. Surgical decompression of impingement in the weight bearing shoulder. Archives of physical medicine and rehabilitation. 1993;74(3):324-327.
[5] Goldstein B, Young J, Escobedo EM. Rotator Cuff Repairs in Individuals With Paraplegia1. American journal of physical medicine & rehabilitation. 1997;76(4):316.
[6] Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Physical therapy. 2000;80(3):276-291.
[7] Lukasiewicz A, McClure P, Michener L, Pratt N, Sennett B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. The Journal of orthopaedic and sports physical therapy. 1999;29(10):574.
[8] Ludewig PM CT, Nawoczenski DA. Three-dimensional scapular orientation and muscle activity at selected positions of humeral elevation. J Orthop Sports Phys Ther. 1996;24(2):57-65.
[9] van der Helm FCT, Pronk GM. Three-dimensional recording and description of motions of the shoulder mechanism. Journal of biomechanical engineering. 1995;117:27.
[10] Wu G vdHF, Veeger HE, Makhsous M, Van Roy P, Anglin C, Nagels J,, Karduna AR MK, Wang X, Werner FW, Buchholz B. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and hand. J Biomech. May 2005;38(5):981-992.
[11] Brose SW, Boninger ML, Fullerton B, et al. Shoulder ultrasound abnormalities, physical examination findings, and pain in manual wheelchair users with spinal cord injury. Archives of physical medicine and rehabilitation. 2008;89(11):2086-2093.
ACKNOWLEDGMENTS
This material is based upon work supported by VA Center grant number B6789C and ASPIRE grant number 1262670. This material is the result of work supported with resources and the use of facilities at the Human Engineering Research Laboratories.
Audio Version PDF Version